





The discovery by Swedish researchers that the SARS-CoV-2 full-length spike protein weakens the adaptive immune system by damaging a crucial DNA repair mechanism raises questions about whether mRNA COVID vaccines could do the same — and whether that might increase a person’s risk of developing cancer.
Intrigued by clinical observations of patients with SARS-CoV-2 which suggested the virus was suppressing adaptive immunity, researchers Hui Jiang and Ya-Fang Mei at the Umeå University in Sweden set out to identify the mechanisms triggering the suppression.
They revealed the results of their findings in a peer-reviewed study, “SARS–CoV–2 Spike Impairs DNA Damage Repair and Inhibits V(D)J Recombination In Vitro,” published in October in the journal Viruses.
Noting the importance of adaptive immunity versus innate immunity, the authors wrote:
“Unlike innate immune responses, the adaptive responses are highly specific to the particular pathogen that induced them. They can also provide long-lasting protection. A person who recovers from measles, for example, is protected for life against measles by the adaptive immune system, although not against other common viruses, such as those that cause mumps or chickenpox.”
The study’s authors used an in vitro cell line to study how the SARS CoV-2 spike protein travels through the body in a person infected with the virus. They reported:
“ … the spike protein localizes in the [cell] nucleus and inhibits DNA damage repair by impeding key DNA repair protein BRCA1 and 53BP1 recruitment to the damage site. Our findings provide evidence of the spike protein hijacking the DNA damage repair machinery and adaptive immune machinery in vitro.”
The researchers acknowledged the discovery was unexpected, stating, “Surprisingly, we found the abundance of the spike protein in the nucleus.”
The nucleus houses the cell’s chromosomes and coordinates all the cell’s activities. One glitch in the DNA of a cell can have devastating downstream effects.
According to the researchers, the DNA repair system and adaptive immune system “are interdependent, especially during lymphocyte development and maturation.”
A loss of function in crucial DNA repair proteins was found to “inhibit the production of functional B and T cells, leading to immunodeficiency,” the authors wrote.


Do we see evidence of immunodeficiency following vaccination?
Clinical trial data from COVID vaccines previously documented abnormalities in a critical part of the body’s immune system — white blood cells production.
The research noted a transient decrease in lymphocytes (T cells and B cells) associated with the Pfizer vaccine and a similar decline in granulocytes (neutrophils) with the AstraZeneca vaccine.
The fact that the Swedish researchers reported a loss of immune function associated with the invasion of the spike protein into the cell nucleus, combined with previous clinical trial data that found transient reductions in the number of white blood cells, may explain reports of increased COVID infections shortly after vaccination.
A preprint study by Public Health England investigating the early effectiveness of vaccination found a “notable” rise in COVID-19 infections in people immediately after they received the Pfizer-BioNTech or AstraZeneca vaccine.
The investigators reported:
“There were significant numbers of vaccinated individuals who go on to develop COVID-19 and our study indicates that vaccinated individuals must maintain other precautions, in particular during the first two to three weeks after vaccination.”
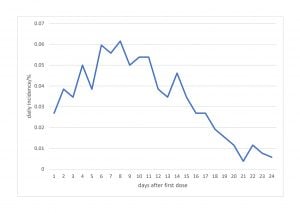
The Public Health England researchers extracted real-world data from the Israel vaccination program and estimated the incidence per day for each day after the first injection and reported a significant spike in cases shortly after vaccination.
They found the daily incidence of COVID infections doubled the first week following vaccination and did not reach the pre-vaccine incidence until 16 days following vaccination. See figure 2:
The authors of an article in The BMJ analyzed the findings of these early vaccine effectiveness studies documenting an increase in COVID infections in the two weeks following vaccination, and concluded “socialization” was responsible for the increased incidence of infection.
But these real-world reports following the launch of the COVID vaccination program globally align with the original Pfizer trial.
Data reported to the U.S. Food and Drug Administration (FDA) by Pfizer found a statistically significant 40% increase in suspected COVID cases, with 409 cases in the vaccinated group in the first week of the trial, compared to 287 in the placebo group.
A group of doctors, scientists, lawyers and other professionals from the UK on Feb. 5 sent an urgent open letter to the Minister for COVID-19 Vaccine Deployment, the Secretary of State for Health and Social Care and two vaccine oversight agencies citing strong epidemiological evidence, from around the world, to support the hypothesis that the COVID vaccine rollout may be linked with increased deaths in certain age groups.
The authors of the letter called for an immediate audit of the deaths following vaccination in the UK.
In their letter, they cited media reports from around the world showing a pattern of outbreaks of COVID and clusters of deaths occurring in the week or two after the vaccine administration, along with statements from national regulators and other official organizations raising serious concerns and calling for investigations.
According to a letter to the editor of The BMJ, commenting on the The BMJ news article that alleged socialization following vaccination was responsible for the increased incidence of infection in the two-week window following COVID vaccination, the UK doctors and scientists wrote:
“Given the evidence of white cell depletion after COVID-19 vaccination from the clinical trial data combined with the findings of and the evidence of increased COVID-19 infection rates shortly after vaccination, the possibility that the two are causally related needs urgent investigation.”
The identification by the Swedish researchers of a molecular mechanism that causes immunosuppression following vaccination only amplifies these concerns.
The critical role of the immune system and DNA repair in preventing cancer
The clinical epidemiologic data supports the Swedish researchers’ finding that immunosuppression caused by the COVID spike protein entering the cell nucleus is a red flag that cancers may also result as an adverse event following COVID vaccination.
The immune system, especially T-cell lymphocytes, is well recognized for the critical role they play in preventing cancer through their constant vigilance in attacking and killing cancer cells before they have an opportunity to develop into a tumor.
In their article, the Swedish researchers did not specifically address injury to the BRAC-1 and 53BP1 repair mechanisms in the cell and its potential to lead to an increased risk of cancer.
But their findings are disturbing given the critical functions these specific two proteins play in protecting the cell from unregulated cell growth.
The BRCA1 protein in the cell is responsible for mending breaks in DNA. It also plays a critical role in maintaining the stability of a cell’s genetic information.
To carry out these functions, the BRCA-1 protein interacts with many other proteins, including other tumor suppressors and proteins that regulate cell division.
The tumor suppressor protein 53BP1 is a pivotal regulator of DNA double-strand break (DSB) repair.
When a cell has a reduced capacity to repair breaks in the DNA, defects accumulate that then trigger cells to grow and divide abnormally resulting in the formation of cancerous tumors.
Mutations in the BRAC1 gene result in a reduction of BRAC1 proteins in the cell. This can lead several high-profile cancers, including breast and ovarian cancer in women and prostate and pancreatic in men.
Mikolaj Raszek, Ph.D., who holds a degree in genetics and a doctorate degree in biochemistry, is concerned about the seriousness of these findings. In a short video he explained the significance of the finding by the Swedish researchers.
Raszek said:
“BRCA1 is mutated, then you have the highest predisposition for cancer development precisely because the BRCA1 gene codes for proteins that fix DNA damage.”
Raszek voiced concerns that we don’t yet know what the vaccines might be doing at the molecular level once injected. He concluded that the consequences are so great that the Swedish study should immediately be replicated and verified.
Biodistribution and persistence of the spike protein
In assessing the potential implications of the Swedish researchers’ findings, it is necessary to identify the biodistribution of the mRNA vaccine lipid nanoparticles which contain the instructions for the cells to manufacture the spike protein.
This information may provide insights as to what tissue and organ systems might be at highest risk for injury.
As The Defender previously reported, Japanese researchers showed lipid nanoparticles from the vaccine did not stay in the deltoid muscle where they were injected, as the vaccine’s developers claimed would happen, but circulated throughout the body.
A Pfizer COVID-19 biodistribution study, obtained by viral immunologist Byram Bridle, showed the lipid nanoparticles that contain the blueprint for the cell to manufacture the spike protein were found in the whole blood circulating throughout the body within four hours.
Dr. Robert Malone, creator of mRNA vaccine technology, joined evolutionary biologist Bret Weinstein, Ph.D., for a three-hour conversation on the “DarkHorse Podcast” to discuss multiple safety concerns related to Pfizer and Moderna vaccines, including the Japanese biodistribution study.
The lipid nanoparticles are the “boxes” the mRNA is shipped in, according to Malone. “If you find lipid nanoparticles in an organ or tissue, that tells you the drug got to that location,” Malone explained.
According to the data in the Japanese study, lipid nanoparticles were found in the whole blood circulating throughout the body within four hours, and then settled in large concentrations in the ovaries, bone marrow and lymph nodes.
Healthy bone marrow is an essential part of the body, as it contains stem cells that produce blood cells and the cells that make up the immune system. The accumulation of the vaccine-generated spike protein in the bone marrow could also explain the immunodeficiency and lower numbers of critical white blood cells following immunization.
“There needed to be monitoring of vaccine recipients for leukemia and lymphomas (also multiple myeloma) as there were concentrations of lipid nanoparticles in the bone marrow and lymph nodes that could trigger these cancers. But those signals often don’t show up for six months to three or nine years down the road.”
SARS -CoV-2 full-length spike protein the culprit
According to Swedish researchers, “only the full–length spike protein strongly inhibited” the two DNA repair mechanisms, BRCA1 and 53BP1, in the cell.
This finding is hugely significant, as the authors noted, because the mRNA and adenovirus vaccines approved for use in the U.S. were developed based on the full-length spike protein.
The researchers wrote:
“Our findings reveal a potential molecular mechanism by which the spike protein might impede adaptive immunity and underscore the potential side effects of full-length spike-based vaccines.”
They further suggested the use of “antigenic epitopes of the SARS-CoV-2” such as receptor-binding domain, or RBD, “might be safer and more efficacious than the full-length spike.”
Scientists voiced concerns about the use of the full-length spike protein in the COVID vaccines even before the vaccines were approved.
For example, in a letter to the FDA in response to a request for public comments during the ‘agencies deliberations to approve the Pfizer vaccine, Dr. Patrick Whelan, M.D., Ph.D., urged caution in approving the vaccine prior to having adequate safety data.
Whelan told the FDA, “It appears that the viral spike protein that is the target of the major SARS-CoV-2 vaccines is also one of the key agents causing the damage to distant organs that may include the brain, heart, lung and kidney.”
Whelan concluded his warning to the FDA with:
“As important as it is to quickly arrest the spread of the virus by immunizing the population, it would be vastly worse if hundreds of millions of people were to suffer long-lasting or even permanent damage to their brain or heart microvasculature as a result of failing to appreciate in the short-term an unintended effect of full-length spike protein-based vaccines on these other organs.”
Given that the full-length spike protein utilized in the currently approved mRNA vaccines has been found to be more injurious than fragments of the protein, and given that it may “hijack” critical DNA repair mechanisms resulting in both a heightened risk of cancer and immunodeficiency, our current vaccine recommendation must undergo extensive scrutiny to assure safety and efficacy.
Critical need for replication of long-term COVID-19 safety studies
Raszek’s statement in the “DarkHorse Podcast” regarding the urgent need to replicate the Swedish researchers’ study because the consequences are so great is paramount.
As Malone said in that same podcast, the development of cancer following injury to the DNA repair mechanisms may take years to manifest.
And vaccines would never be identified as the culprit without robust long-term monitoring of all health outcomes — not just COVID infection — following vaccination.
Follow-up after vaccination must also include monitoring a robust control group of individuals who did not receive the vaccine.
However, during the clinical trials for both the Pfizer and Moderna vaccines, individuals who initially received the placebo were subsequently allowed to take the vaccine, which destroyed the opportunity for long-term follow-up of all health outcomes in those who did not receive the vaccine.
The fact that COVID vaccines are being recommended for everyone, and in some cases mandated by employers, will essentially make such studies impossible to conduct.
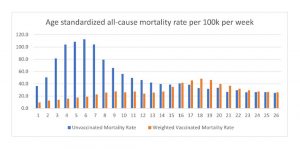
Despite the fact that we currently lack long-term safety data, recent findings have emerged from England that document all-cause weighted mortality data for vaccinated individuals has steadily increased to the point where the death rate is currently higher among the vaccinated than unvaccinated.
The age-adjusted mortality rates for vaccinated compared to unvaccinated for weeks one to 26 of 2021 are charted below using data generated by Norman Fenton, Ph.D., a risk information management professor, and Martin Neil, Ph.D., a computer science and statistics professor. Both are affiliated with Queen Mary University of London.
Overall, the chart shows that, over time, the weighted mortality rate for the vaccinated has steadily increased and by week 16 (April), surpassed that for the unvaccinated.
Given that the U.S. follows similar vaccine policies, it is only logical to assume the same scenario is playing out here.