





By Harvey Risch
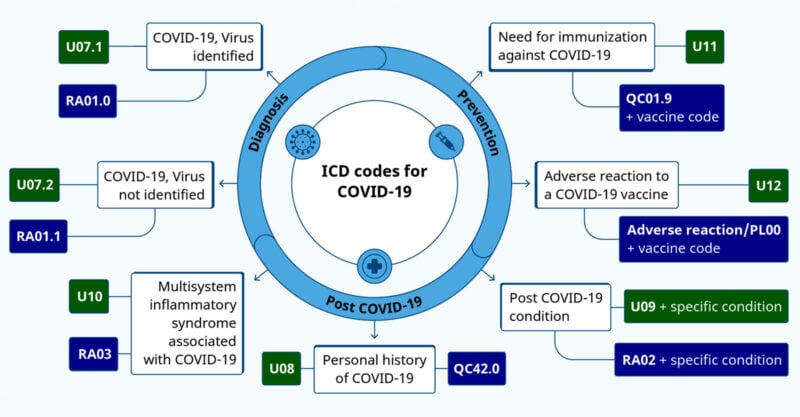
The Centers for Disease Control and Prevention (CDC) recently codified International Classification of Disease (ICD) codes for COVID-19 vaccine status.
ICD codes are extensively used in medical records, medical insurance data and health research to classify precisely disease states as well as injuries from exogenous agents such as accidents, medication and medical device injuries, toxic chemicals, etc.
Vaccination status is not a disease or an injury state, yet CDC has rationalized creating ICD codes for it. The coding is set to become effective on April 1.
As described by Dr. Robert Malone, “The ICD classification system is run by the World Health Organization, not the U.S. government.”
The vaccine status ICD codes were developed by the U.S. Centers for Medicare and Medicaid Services some nine months ago, and CDC is implementing them.
The coding scheme, Z28.xxx, includes both vaccination status and possible reasons for the status. However, there does not appear to be a code for “fully vaccinated,” only for various states of “not fully vaccinated.”
- The code Z28.0 means “immunization not carried out because of contraindication.” Z28.1 means “immunization not carried out because of patient decision for reasons of belief or group pressure.”
- Z28.2 means “immunization not carried out because of patient decision for other and unspecified reason.”
- Z28.8 means “immunization not carried out for other reason” which because of code Z28.2 must refer to reasons not attributable to patient decisions.
- Finally, Z28.39 means “other underimmunization status,” including “Delinquent immunization status” and “Lapsed immunization schedule status.”
However, a potential contradiction arises because code Z28.310 means “unvaccinated for COVID-19.” In order to reconcile this, the Z28 codes in the previous paragraph must refer to vaccines other than for COVID-19.
The only other COVID-19 code is Z28.311 which means “partially vaccinated for COVID-19,” where “partial” refers to the CDC definition for “fully vaccinated” at the time when the patient visits the healthcare provider who records the vaccination status in the medical chart.

It is apparent that the details of reasons for patient choices for vaccine status are not specified in codes for COVID-19 vaccines, but the CDC has some two months to fix this.
There are no specific codes yet for “refused to divulge COVID-19 vaccination status” or “unknown COVID-19 vaccination status,” but these codes are likely to be added at some point.
What is the usage for which this information is planned?
There is certainly a public health rationale for agencies to be able to monitor population vaccination status. Personal health information is routinely analyzed by public health agencies, insurance companies and health researchers, but in anonymized and grouped formats.
The identifiable information is recorded in the databases, however HIPAA and other laws strictly protect identifiable health information and regulate how such information may be used for analyses.
In theory, vaccination status could be no different. Medical records already know your age, gender and race, where you reside, about your obesity, diabetes, your smoking and alcohol usage and your HIV status.
Some of this information could be stigmatizing if released publicly, but at present there are no politicized or other circumstances to force unwanted choices on members of the public based on this compiled personal information.
Imagine, however, that one day, government agents are pounding on your door at 6 a.m., telling you that you are required to take smoking cessation medications, under penalty of forced residence in a “smoking-cessation hotel” until you submit to the government’s requirement.
The medications have built-in transmitters that are activated when exposed to stomach acid, so taking them is recorded.
After all, 500,000 Americans die every year from smoking-related diseases and their end-of-life medical care is an expense for which the government no longer wants to pay.
Your smoking is economically hurting the medical care that grandma needs. Or something.
But COVID-19 and its vaccination are different.
The COVID-19 vaccines and their boosters were created under emergency-use authorization, or EUA, protocols and are not fully licensed. The Biologics License Application versions, e.g., Comirnaty, are not generally available in the U.S.
This licensing chicanery has not gone unnoticed by the American public and a substantial fraction of people find the vaccines controversial.
Many people have seen their multiple-vaccinated friends and relatives get COVID-19, some multiple times. Many have also seen friends and relatives harmed by the vaccines, and most people know of the incessant daily deaths of healthy athletes, deaths discussed as caused by “coincidence.”
People have seen the vaccines touted as solutions to the pandemic, yet utterly fail across the population to suppress transmission of the infection.
And, people have been bombarded with daily narratives for two solid years that the vaccines are “safe and effective” and that they must be taken, and that unvaccinated people are “bad,” “selfish,” demonized as doing damage to society and should be shunned.
That is, personal vaccination status today is the most stigmatizing personal data of modern times, surpassing having AIDS. As such, any government compilation must be “bulletproof” against hacking and misuse.
As well, the government must be trusted to maintain the data for use only as other personal medical data have been used.
Given the two-plus years of massive government propaganda about the vaccines, about their adverse effects, about COVID-19, about early COVID-19 treatment and the government collusion with social media companies in suppression of valid dissenting medical and scientific opinions and data, there is no empirical reason to support trusting the government with such sensitive, stigmatizing data.
There is no reason to believe that the government will not release the status information to insurance companies or other companies doing large business with the American public.
Further, there is no recourse should the government actually release such confidential data.
Thus, nothing may stop such companies from restricting activities based on the stigmatized data. For example, public travel could be blocked; bank accounts could be blocked; purchasing could be blocked.
The free pursuit of happiness is enshrined in our Declaration of Independence. The government cannot lawfully interfere with normal transactions of everyday life. But private companies working at the government’s behest, with government-supplied personal status information, could very well do it.
As has been seen from the Freedom of Information Act, or FOIA, documents, hundreds of government employees have spent the pandemic years doing exactly this unconstitutional behavior in getting social media companies to suppress Americans’ freedom of speech.
Furthermore, there is now no rational government interest in compiling vaccination status at all. At a time when vaccination was generally thought (incorrectly) to reduce COVID-19 transmission across the population, there might have been a rationale for doing so.
However, on Aug. 11, 2022, the CDC stated publicly that the COVID-19 vaccines do not work as a public health measure to control virus transmission.
They said, “Receipt of a primary series alone, in the absence of being up to date with vaccination* through receipt of all recommended booster doses, provides minimal protection against infection and transmission (3,6).” “Being up to date with vaccination provides a transient period of increased protection against infection and transmission after the most recent dose, although protection can wane over time.”
The fact that such benefit is “transient” and wanes implies that after some short period, boosters fail to reduce risk of transmission and thus that vaccine mandates are invalid.
The only government interest in mandating COVID-19 vaccines, and thus in compiling personal information about vaccination status, is that the vaccines reduce transmission.
They don’t.
Secondly, the CDC’s August 11 policy guidance does not distinguish between vaccinated and unvaccinated people in any way for any policy. There is thus no compelling government purpose in defining people as vaccinated or unvaccinated.
It would be like the government compiling personal information on hair color, except that hair color is not stigmatizing and vaccination status is extremely stigmatizing.
The government itself — through the CDC — has determined that vaccination status is not of policy importance. There can thus be no compelling interest for the government to forcibly collect this information against the wishes of the population, even were it not stigmatizing.
So much more so after the government has spent the last two years publicly demonizing unvaccinated people for their rational and legitimate personal health choices.
Originally published by Brownstone Institute.
Harvey Risch, senior scholar at Brownstone Institute, is a physician and a Professor Emeritus of Epidemiology at Yale School of Public Health and Yale School of Medicine. His main research interests are in cancer etiology, prevention and early diagnosis and in epidemiologic methods.
