






Editor’s note: This article is Part 2 in a series exploring vaccine clinical trials. Read Part 1 here.
As Edward H. Kass, Harvard physician and founding member and first president of the Infectious Disease Society of America, stated in 1971 in an article published in The Journal of Infectious Diseases:
“We had accepted some half-truths and had stopped searching for the whole truths. The principal half-truths were that medical research had stamped out the great killers of the past — tuberculosis, diphtheria, pneumonia, puerperal sepsis, etc. — and that medical research and our superior system of medical care were major factors in extending life expectancy.
“The data on deaths from tuberculosis show that the mortality rate from this disease has been declining steadily since the middle of the 19th century and has continued to decline in almost linear fashion during the past 100 years [till 1970].
“There were increases in rates of tuberculosis during wars and under specified adverse local conditions. The poor and the crowded always came off worst of all in war and in peace, but the overall decline in deaths from tuberculosis was not altered measurably by the discovery of the tuberculosis bacillus, the advent of the tuberculin test, the appearance of BCG vaccination, the widespread use of mass screening, the intensive anti-tuberculosis campaigns, or the discovery of streptomycin. It is important that this point be understood in its completeness.
“The point was made years ago by Wade Hampton Frost, and more recently by René Dubos, and has been repeatedly stressed through the years by many observers of the public health. Similar trends in mortality have been reported with respect to diphtheria, scarlet fever, rheumatic fever, pertussis, measles, and many others.”
Anthony R. Mawson, Professor of epidemiology and biostatistics, took the same line in 2018 when he stated: “It is well known that deaths from common infectious diseases declined dramatically before the advent of most vaccines due to improved environmental conditions — even diseases for which there were no vaccines.”
In this context, we would also like to briefly refute Jess Steiner’s assertion that Salk’s polio vaccine made “cases dropping from 58,000 (1957) to 161 (1961).”

From 1923 to 1953, long before large-scale polio vaccinations began to be carried out in the mid-1950s, mortalities attributed to polio had already decreased substantially: In the USA by 47 percent; in Great Britain by 55 percent; in other European countries, the statistics are comparable. This diagram was reproduced with permission from the following book: Vaccines: Are They Really Safe and Effective? © Neil Z. Miller.
On the one hand, this does not invalidate the data presented in Miller’s graph (see above) showing that Salk’s polio vaccine has nothing to do with the containment of polio.
On the other hand, it is also important to bear in mind that the standards for defining polio were changed in 1955, causing the number of polio diagnoses to drop noticeably.
According to scientific journalist Neil Miller:
“The new definition of a ‘polio epidemic’ required more cases to be reported. Paralytic polio was redefined as well, making it more difficult to confirm and tally cases. Prior … the patient only had to exhibit paralytic symptoms for 24 hours. Laboratory confirmation and tests to determine residual (prolonged) paralysis wer not required.
“The new definition required the patient to exhibit paralytic symptoms for at least 60 days, and residual paralysis had to be confirmed twice during the course of the disease. Also, [from then on] … cases of aseptic meningitis … and coxsackie virus infections were reported as separate diseases from polio. But such cases were counted as polio before …
“In 1976, Dr. Jonas Salk, creator of the killed-virus vaccine used in the 1950s, testified that the live-virus vaccine (used almost exclusively in the United States from the early 1960s to 2000) was the ‘principal if not sole cause’ of all reported polio cases in the U.S. since 1961.”
So what caused the polio ‘epidemic?’
There are many indications that not only are vaccines to blame, but especially toxins such as DDT (see diagram below).
In the Philippines, only a few years before the Salk vaccine disaster in the U.S., the first polio epidemic in the tropics occurred spontaneously, in fact, with the introduction of the insecticide DDT there.
Around the end of World War II, U.S. troops in the Philippines had sprayed masses of DDT daily to wipe out flies. Just two years later, the well-known Journal of the American Medical Association reported that lameness among soldiers stationed in the Philippines could not be differentiated from polio, and it had advanced to become the second most common cause of death.
Only combat exercises were said to have claimed more victims. Meanwhile, populations in neighboring areas, where the poison had not been sprayed, experienced no problems with paralysis.

A look at statistics shows that the polio epidemic in the United States of America reached its peak in 1952, and from then on rapidly declined. We have seen that this cannot be explained by the Salk-inoculation, since this was first introduced in 1955. There is a most striking parallel between polio development and the utilization of the severe neurotoxin DDT and other highly toxic pesticides. Sources: West, Jim, Pesticides and Polio, Townsend Letter for Doctors and Patients, June 2000, p. 68-75; West, Jim, Images of Poliomyelitis; Handbook of Pesticide Toxicology, Eds.: Hayes, Wayland; Laws, Edward, Academic Press Inc., Harcourt Brace Jovanovich, Publishers, San Diego, 1991, p. 769; Historical Statistics of the US (1975), US Government Printing Office; Scobey, Ralph, Is Human Poliomyelitis Caused By An Exogenous Virus?, Archives of Pediatrics, 1954. © Jim West.
Merck didn’t use true placebo in Gardasil trials
The approval trial of the cervical cancer (HPV) vaccine Gardasil is also cited by public health scientist Dr. Jess Steier as a successful example of a placebo study.
In this study, no placebo in the form of a saline solution was taken, but an “active comparator” riddled with aluminum was used. In this context, it is being claimed — also by Steier, for example — that the “aluminum adjuvant system was already proven safe and necessary for the vaccine to work.”
But the opposite is true. “Gardasil” which was designed to prevent cervical cancer and genital warts in sexually active women, has not been proven safe and effective in clinical trials. In fact, the vaccine triggered adverse event reports in 90% of the test subjects within 15 days — hardly an indication of safety.
However, the controversial aluminum-containing “placebo” formula triggered 85% of the adverse event reports. This raises reasonable concerns about accurately distinguishing vaccine-induced side effects from those caused by the adjuvant.
Without an untreated null group, genuine safety profiles remain elusive. Moreover, the U.S. Food and Drug Administration doesn’t know what long-term adverse effects the vaccine might produce. In fact, Gardasil comes along with heavy side effects ranging from reddening and swelling around the injection site, fever, hives, arthritis and even death.
Apart from that, according to the 2018 Cochrane review on HPV vaccines, which analyzed data from over 73,000 participants in 26 studies, the vaccination did not reduce rates of invasive cervical cancer or overall mortality. It only showed reductions in surrogate markers — specifically, cervical intraepithelial neoplasia (CIN2+ and CIN3+), which may regress spontaneously and are not equivalent to cancer.
These so-called “precancerous lesions” are often detected through invasive screening and lack proven clinical relevance. As such, the claimed preventive effect on cervical cancer remains absolutely speculative.
And that’s not all. A recently published expert report by Dr. Peter C. Gøtzsche, Danish medical researcher and co-founder of the Cochrane Collaboration, accuses Gardasil maker Merck in connection with a U.S. lawsuit of falsifying Gardasil trial data, concealing serious side effects and deceiving the regulatory authorities.
According to the report, the studies financed by Merck are not suitable for correctly assessing the negative effects of the vaccine.
COVID vaccines don’t meet the placebo-controlled standard, either
The COVID-19 “vaccines” — about which even Stefan Oelrich, member of the Board of Management of Bayer AG, stated that it is not a classical vaccine (the so-called mRNA injections penetrate cells and only cause certain cells to produce antibodies) — are also being named as positive examples of placebo-controlled studies.
However, these studies have several fundamental shortcomings. COVID-19 trials were only “observer-blinded,” meaning healthcare providers administering the vaccines knew who received the vaccine and who received placebo, introducing potential biases into data collection and interpretation.
Additionally, the blinding within these studies was lifted after approximately two months, transitioning participants into an open-label phase, further limiting the ability to assess long-term efficacy and safety due to potential bias in data collection and interpretation.
Noteworthy in this context is the “Forensic Analysis of the 38 Subject Deaths in the 6-Month Interim Report of the Pfizer/BioNTech BNT162b2 mRNA vaccine clinical trial,” compiled by the DailyClout Pfizer/BioNTech Documents Investigations Team.
The analysis states:
“The analysis reported here is unique: It is the first study of the original data from the Pfizer/BioNTech BNT162b2 mRNA vaccine clinical trial (C4591001) to be carried out by a group unaffiliated with the trial sponsor.
“Key findings include that of the 38 deaths reported in the 6-month interim adverse event report, 21 subjects vaccinated with the Pfizer/Biontech BNT162b2 injection died compared to 17 placebo subjects. The number of cardiac events was 3.7-fold higher in subjects who received the BNT162b2 vaccine compared to placebo.”
What about the trials that went wrong?
Meanwhile, it is remarkable that people like Steiner fail to mention crucial placebo studies showing that the vaccines came off badly. One of the most famous examples of this is a large-scale field trial that the WHO implemented in India at the end of the 1960s, on the BCG vaccine (for tuberculosis).
In this trial, “a large collective was vaccinated with BCG, while an equally large one remained unvaccinated.” The results: Not only did the vaccination show no protective effect against tuberculosis, but significantly more participants fell ill and died in the vaccinated group compared to the unvaccinated group.
Another rare example of a properly controlled trial stems from 2012, in which an influenza vaccine was compared with a true placebo in children. The result was devastating. Despite the authors trying to support influenza vaccination, they admitted: “There was no statistically significant difference in the risk of confirmed seasonal influenza infection” between the groups. Even worse: the vaccine group “had higher risk of acute respiratory illness,” with non-influenza infections.
Against this background, the question arises why the Trump government indicated its plan to make placebo trials for every “new study” compulsory wouldn’t apply to the flu vaccine, which is updated year to year and which, according to the HHS, “has been tried and tested for more than 80 years.”
Flu vaccines are manufactured before the (claimed) viruses they are supposed to work against even exist. And as if that weren’t enough, on close examination of the flu data upon which the warnings of the “epidemic hunters” from the CDC, RKI or WHO are based, the question crops up: “Are U.S. flu death figures more PR than science?”
This is precisely the title of a study published in 2005 in the British Medical Journal. The author, Peter Doshi, Ph.D., associate professor at the University of Maryland School of Pharmacy and senior editor at The BMJ, provided a resoundingly decisive answer: “US data on influenza deaths are a mess.”
Doshi’s main criticism is that the CDC works under the assumption that 36,000 Americans die from viral flu each year — but they still owe us proof that an influenza virus really kills these people. Doshi’s conclusion: The CDC’s communication strategy is equivalent to “marketing of fear.”
Several astute observers critiqued the government’s promotional campaign urging the public to vaccinate against the flu by challenging the 36,000 annual death count the CDC attributes to the flu. Especially worth mentioning is the meta-analysis of the published flu vaccine reports by Tom Jefferson of the Cochrane Center. The findings of these 2006 articles are sobering: A major gap exists between evidence and public health policy.
Antibodies don’t reliably predict immunity
Steier also cites a placebo trial on the measles vaccine, namely a study from Israel published in 1968 and with the title “A Comparative Study of Four Live Measles Vaccines in Israel.”
In this trial, children in the vaccine group were divided into four subgroups, each receiving one of the four different vaccines. The remaining children were assigned a saline placebo. And according to Steier, the result was that the vaccines are ”safe and effective compared to placebo.”
But how she comes to this conclusion will probably remain her secret. In fact, in the study we can read:
“Febrile reactions of ≥ 37.50 °C in the different treatment groups varied from 86.4% in the Enders Edmonston group to 63.1 % in the Moraten group and 51.2% after placebo inoculation. The incidence of fever was always in the same relative order: Enders Edmonston > Beckenham > Schwarz > Moraten > Placebo … The incidence of rash … was greatest in the groups inoculated with Enders Edmonston and Beckenham vaccines (36.4% and 36.9%); it was less in the group given Schwarz vaccine (28.4%) and lowest (20.2 %) in those given Moraten vaccine.
“In the placebo group, rash was recorded in 11.9% of the children … The 4 vaccines can be listed as follows in decreasing order of the fever (≥ 37.50 °C) induced: Enders Edmonston (86.4 %), Beckenham (78.6 %), Schwarz (66.7 %) and Moraten (63.1 %). The same decreasing trend was seen when pyrexias of > 38.30C and >40’C were considered. It should be noted, however, that such temperatures were also recorded in the placebo group, though to a lesser extent.”
The only possibility that could have led Steier to conclude that the measles vaccine is “safe and effective compared to placebo” is that she refers to seroconversion. This is the phase of a vaccination or infection in which specific antibodies against antigens of a foreign body (claimed virus, for example) are detectable in the blood serum for the first time. A high seroconversion is believed to be a good sign. And the numbers of seroconversions determined in the study are:
“92.7% after Beckenham vaccine, 97.1% after Schwarz vaccine and 100% after Enders Edmonston and Moraten vaccines. In each of the cases of seroconversion a 4-fold or greater rise in antibody titre was observed. In addition, 3 of the 37 children given placebo reacted with high seroconversion titres. Since clinical measles was not observed in these cases, and since measles was not prevalent at the time, one possible explanation is that these children were inoculated by mistake with vaccine and misrecorded.”
But another explanation for the observation that 3 of the 37 children given placebo reacted with high seroconversion titres would be that so-called surrogate markers, such as antibody tests, are not reliable and react to all kinds of things.
In fact, the magazine Impf-report found that even the federal authorities have been unable to provide evidence that there is a health benefit for people who have a high antibody titer. And even various orthodox sources confirm that the amount of so-called antibodies in the blood does not reliably predict a person’s immunity.
The unbeatable proof that there is no proof that the measles vaccine was useful, meanwhile, is also evident from the historical data, as explained by Kass and Mawson, for example:
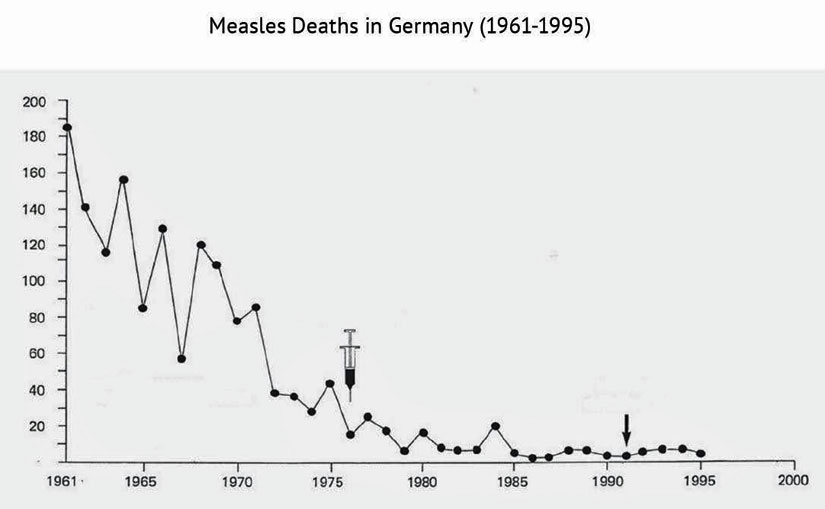
Measles vaccination was introduced in West Germany in the mid-1970s (where the syringe is shown in the graphic), at a time when the “measles scare” was essentially over. The arrow (early 1990s) indicates the combined the data from reunited Germany. Source: Gerhard Buchwald. Impfen: Das Geschäft mit der Angst (in English: Vaccination: a Business based on Fear), Knaur, 1997, p. 133. Data basis comes from the German Federal Statistical Office.
How should we move forward?
It is one of the fundamental problems of our times that vaccine trials (as well as many, many other studies on drugs) often primarily rely on surrogate markers such as “antibody titers” or PCR test results instead of directly measurable clinical outcomes such as symptom resolution, functional improvement, or mortality reduction.
This has already been criticized in connection with the Salk/Francis polio vaccine study. M. Beddow Bayly stated that “the conclusion is not justified that the presence of a high antibody titre in human b/cod or serum indicates that protection against poliomyelitis infection has been established.”
Bayly wrote:
“The fallacy of the assumption that antibody formation is a measure of immunity was fully demonstrated in a Report issued by the Medical Research Council in May 1950, entitled, ‘A Study of Diphtheria in Two Areas of Great Britain.’ In this report by nine doctors (Percival Hartley. W. J. Tulloeb, M.Anderson. W. A. Davidson, J. Grant, W. M. Jamieson, C. Kenbarrer. R. Morton, and G. H. Robertson) it was stated that the occurrence of diphtheria in the inoculated led to the investigation into the immunity state and the behaviour of the immunity mechanism.”
The evidence is overwhelming that such surrogate markers do not necessarily translate into meaningful health benefits. In the BionTech/Pfizer COVID-19 vaccine trial, symptomatic cases without positive PCR tests (“suspected COVID-19 cases”) were excluded, significantly distorting efficacy results. Inclusion of these cases could have eliminated observed effectiveness differences between vaccine and placebo groups.
At this point, it should also be emphasized that, though the whole world relied on RT-PCR to “diagnose” SARS-CoV-2 infection, the science is clear: These tests are not fit for purpose. In fact, COVID-19 PCR Tests can be labeled as “scientifically meaningless” in the context of detecting viruses and viral infections.
Even Dr. Anthony Fauci conceded to MSNBC in late December 2021: “PCR doesn’t measure replication competent virus … The only way you can tell if it‘s transmissible [is] if you can show that there really is life replication virus in you — and the tests [= PCR and antigen tests] don’t measure that.”
As far as the measles vaccine is concerned, there is another question that arises: Why was it not tested against placebo when it was introduced? In other words: Why were several measles vaccines only tested against a placebo in Israel in 1968 and not as early as 1960, when John Enders meant to have tested the world’s first measles vaccine for its usefulness in his paper published in the New England Journal of Medicine?
That is to say, the “ethical argument” does not apply here either, as it states that if an effective treatment already exists, it is unethical to give participants a placebo because they are being deprived of an effective treatment. But if Enders did not test his measles injection againsta placebo, it is impossible to conclude that doing nothing is or was superior. Hence, also in the case of the measles vaccine, the widely applied principle described by Steier is thus also reduced to absurdity. It reads:
“If we’re testing a new measles vaccine, giving half the children a saline placebo would leave them vulnerable to a potentially deadly disease when a proven vaccine already exists. Instead, researchers compare the new vaccine to the current standard to prove it’s at least as safe and effective.”
By the way, it is also important to bear in mind that a proper placebo control, scientifically speaking, should differ from the vaccine in only one factor: the hypothesized active component. Using saline solution alone does not fulfill this requirement, as it differs from the vaccine in several variables — not only in the so-called viral component, but also in chemical composition, biological impact, and pharmacological activity. Therefore, saline is not a 100% valid negative control if the goal is to isolate the effect of the viral component specifically.
A better approach would be to use a placebo that matches all components of the vaccine formulation except the so-called independent variable — the viral element — thereby fulfilling the definition of a scientific negative control. Furthermore, an additional untreated null group is essential to assess placebo effects and the natural course of illness without intervention. A true placebo control should match all vaccine components except the intended active viral component.
An additional critical element typically missing from vaccine trials is the inclusion of a null group — a cohort receiving no intervention whatsoever. This group is essential to accurately assess the natural progression of illnesses and fully account for placebo effects. Without a genuine untreated control group, interpreting safety and efficacy data remains inherently problematic.
Lastly, rigorous scientific evaluation demands we consider both relative and absolute risk reductions. Currently, vaccine trials frequently emphasize relative risk reductions, misleadingly exaggerating vaccine effectiveness, especially when the actual number of cases is small.
Providing absolute risk figures alongside relative risks would greatly enhance transparency and practical relevance.
Kennedy’s demand for placebo-controlled studies represents a valuable step toward more rigorous scientific scrutiny of vaccines. And he cannot be given enough credit for having the courage to initiate such a measure in an environment dominated by Big Pharma for many, many decades and with mainstream media that often enough come across as the mouthpiece of Big Pharma.
As the New York Times journalist Natalie Angier put it in 1991: “We science journalists, perhaps more than any other class of reporters, too often serve as perky cheerleaders for our subject and our sources.”
However, if we are aiming for ideal conditions and science that is unrivaled in soundness, reforms should include complete double-blinding, defined clinical endpoints, genuine placebo controls, untreated null groups, and transparent reporting of both relative and absolute risk reductions.
Moving forward, embracing comprehensive standards will be essential for truly transparent, scientifically robust vaccine research.

