






By Chimnonso Onyekwelu and Meleni Aldridge
In just 20 years, the number of children and young people with high blood pressure, or HBP, has nearly doubled. Once seen as an adult problem, it now shows up in classrooms, playgrounds and routine pediatric visits.
According to The Lancet Child & Adolescent Health, prevalence rose from 3.4% in 2000 to 6.5% in 2020 — over 114 million young people affected. This surge begs a question: are kids truly sicker, or are we simply casting a wider diagnostic net?
A key turning point came in 2017 when the American Academy of Pediatrics (AAP) updated its guidelines. The new rules simplified blood pressure categories for teens and aligned thresholds more closely with adults. Millions of previously “healthy” teens instantly moved into “at-risk” or hypertensive groups.
Guidelines tell only part of the story. Children’s diets, sleep, stress, activity levels and environments have shifted dramatically.
While some HBP stems from medical conditions like kidney or heart problems, endocrine disorders, diabetes or family history, research consistently points (here and here) to overweight, poor diets, physical inactivity and sedentary lifestyles as the main drivers in older children.
With blood pressure rising so sharply, shouldn’t prevention take as much priority as treatment? Too often, new drugs arrive faster than efforts to stop children from becoming unwell in the first place.
We explore what high blood pressure means in childhood, how guideline changes have widened diagnostic categories, the known causes and consequences, and practical, natural ways to help lower a child’s blood pressure — and keep it there.
Understanding high blood pressure and the expanding diagnostic net
Simple, HBP, or hypertension, occurs when the force of blood against artery walls remains consistently elevated. Over time, this extra strain forces the heart to work harder, increasing the risk of long-term complications such as heart and kidney disease.
In children, hypertension may be silent, often discovered only during routine check-ups, yet its effects can quietly set the stage for lifelong cardiovascular problems.
The 2017 AAP Clinical Practice Guideline marked a major shift from the 2004 Fourth Report. Among adolescents aged 13 and above, the guideline abandoned percentile-based thresholds, adopting fixed adult cut-points (≥120/80 mm Hg for elevated blood pressure and ≥130/80 mm Hg for hypertension).
It replaced “prehypertension” with the broader “elevated blood pressure” label and recalculated percentiles using only normal-weight children, effectively lowering thresholds for younger children.
These changes may have simplified the diagnosis, but also mean that more children now cross the threshold into elevated or high blood pressure ranges.
The impact is striking. A 2023 study shows that under the 2017 guidelines, the prevalence of hypertension in adolescents rose from 8.4% to 12.9%, elevated blood pressure from 6.1% to 13.8%, and overall HBP from 14.5% to 26.7%.
Another analysis found that Stage 1 hypertension increased from 6% to 10%, and Stage 2 from 0.5% to 1% under the updated criteria. Even among children ages 6-12, HBP classification jumped from 10.8% to 16.7% with the 2017 tables (research here and here).
While these numbers partly reflect guideline changes rather than an abrupt rise in illness, they show how redefining “normal” can suddenly label millions of otherwise healthy children as needing monitoring and intervention.
Other drivers of high blood pressure in children
Apart from the apparent rise caused by the 2017 AAP guideline, several well-established factors directly contribute to high blood pressure in children and young people.
At the center of this is obesity — consistently identified as the strongest predictor of blood pressure rising above the 90th or 95th percentile (the cut-offs for elevated blood pressure and hypertension).
Multiple studies (here and here) have shown that obesity alone significantly increases a child’s risk, with more than 30% of obese boys (and up to 42% in some ethnic groups) and 23–30% of obese girls meeting the criteria for high or borderline blood pressure.
A large meta-analysis also found that obese children were six times more likely to have elevated blood pressure than those of normal weight, while school-based research showed that students at risk of overweight had noticeably higher rates of HBP than their peers.
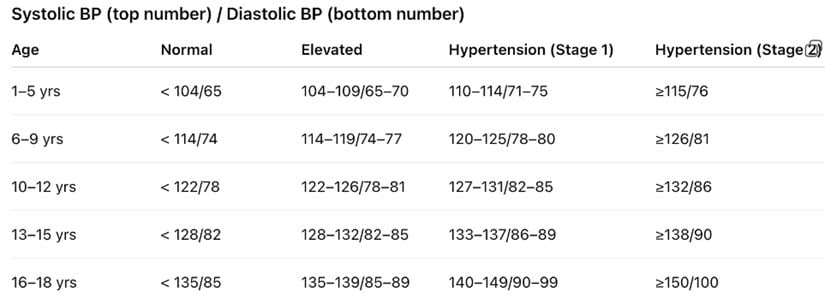
A guide to children’s blood pressure
Physical inactivity and long hours of sedentary behaviour add another layer of risk. Children who do not meet the recommended minimum 60 minutes of daily activity, or who sit for more than two hours a day, show higher rates of both pre-hypertension and hypertension during follow-up.
Diet plays a similar role: high-sodium foods, processed and ultraprocessed meals, sugary drinks and low intake of fruits, vegetables and fiber all contribute indirectly by promoting weight gain and raising long-term cardiovascular risk.
Poor sleep quality and sleep-related breathing problems also play a part, especially in children who are already overweight.
There are also medical causes that, while less common, are important to recognize. These include kidney disease, congenital or acquired heart problems, thyroid or adrenal disorders, diabetes, inherited conditions and even chronic stress.
In such cases, high blood pressure can appear regardless of weight, making proper evaluation essential when readings persist above the expected percentile ranges.
The hidden toll of hypertension in childhood
HBP in childhood is not a temporary phase that children “grow out of.” Research (here and here) consistently shows that children with raised systolic readings have a three- to fourfold higher likelihood of becoming hypertensive adults.
One study following individuals from early childhood into their 30s found that those who later developed metabolic problems had significantly higher blood pressure levels in childhood than their peers.
Hypertension remains the most widespread non-communicable disease globally, and its earliest footprints are often laid down long before adulthood. Elevated blood pressure in young people already increases their future risk of heart attack, stroke and kidney disease — conditions once thought to belong only to older age.
The structural effects on the body begin alarmingly early. In one study of 130 children and adolescents with blood pressure above the 90th percentile, only 45% had a normal heart muscle size, while 14% had severe thickening linked to a fourfold rise in cardiovascular complications in adults.
Other early warning signs — higher urinary albumin, retinal vessel changes, subtle cognitive impacts and early atherosclerotic changes — have also been reported.
Short-term risks can be just as concerning, including persistent headaches, vision disturbances, vomiting, seizures and silent kidney strain. All of this confirms that childhood HBP is far from harmless; it is an early signal of a body already under pressure.
Practical and natural ways to lower blood pressure in children
It is worrying that a condition once seen almost exclusively in adults is now showing up in children and at such alarming rates.
Somewhere along the way, we normalized reaching for medication before addressing the root causes, even in young people whose bodies are still developing.
Children should not be carrying the burden of diseases driven largely by modern lifestyles, nor should drugs become the default solution for every health concern. We owe them better than that. Especially when in many cases, HBP — and the creation of chronic disease — is wholly preventable.
So how do we begin to turn the tide and support children in ways that strengthen health rather than simply manage disease?


Below are practical, research-supported steps to help reclaim a child’s health:
Weight reduction (if overweight or obese): For obesity-related hypertension, even modest weight loss can significantly lower blood pressure.
Begin with gradual, sustainable adjustments rather than strict or restrictive diets and pay close attention to the possibility of emotional eating patterns. See ANH’s Food4Kids guidelines for more information and further articles here, here and here.
Daily physical activity: Children should be active. It’s their natural evolutionary norm. Sedentary behaviour is not and will not result in pathology. Aim for a minimum of 60 minutes of moderate to vigorous activity most days.
Sports, brisk walking, cycling — anything that raises the heart rate counts and most importantly, is fun! Active, fun play is something that has largely been replaced with digital devices, but is far more important than many parents might realize.
Active play influences brain structure, neurological processes and emotional resilience as well as lowering blood pressure and insulin levels and promoting better metabolic health (see studies here, here and here).
Reduce sedentary time: Closely linked to the previous point is the need to limit screen-based activities to less than two hours a day to lower blood pressure and improve overall metabolic health.
A child’s brain develops and enhances higher executive function through physical activity, play and learning how to successfully solve their own challenges. None of this happens in front of a digital screen.
Stress management: The effects of stress and trauma are insidious and affect the entire body, given that the whole immune system is activated. The body doesn’t differentiate between physical or emotional wounding.
In children who are rapidly growing, developing and laying down the neuronal circuitry that will form the foundation for how they respond to challenges through life, managing stress is essential.
Storytelling, breathwork and mindfulness practice, along with physical activity out in nature, can be useful antidotes. Helping children to recognize, feel and process their emotions versus ignoring them, stuffing them deep inside or eating to drown them out, will reap myriad benefits throughout life.
Heart-healthy diet: Increase the child’s intake of fruits, vegetables and fiber, whilst ensuring sufficient healthy fats and protein. Limit dairy intake if they show signs of intolerance and replace sugary and fizzy soda drinks with water. See ANH’s Food4Kids guidelines for more information and further articles here, here and here.
Avoid ultraprocessed foods: Limit packaged snacks, fast food, sweetened cereals and processed meats. These are high in sodium, sugar and unhealthy fats that can raise BP and contribute to weight gain. Choosing whole or minimally processed meals makes a noticeable difference.
Better sleep practices: Ensure children have the required number of hours of uninterrupted sleep in a pitch-dark room daily. This enhances cellular regeneration, gives the brain adequate rest to promote neuronal health and helps to address sleep issues early, as poor sleep can elevate blood pressure.
The American Academy of Sleep Medicine and the AAP concur on the following number of hours of sleep for healthy children:
- Infants (4-12 months): 12-16 hours (including naps)
- Toddlers (1-2 years): 11-14 hours (including naps)
- Preschoolers (3-5 years): 10-13 hours (including naps)
- School-age children (6-12 years): 9-12 hours
- Teenagers/adolescents (13-18 years): 8-10 hours
Family-based approaches: Children thrive when the entire family adopts healthier habits together. Shared meals, shared activity, fun, laughter and consistent routines dramatically improve outcomes.
Originally published by Alliance for Natural Health International.
Chimnonso Onyekwelu serves as a legal researcher at Alliance for Natural Health International, where she does high-level policy analysis and interpretation of legal frameworks in the health and nutrition sector.
Meleni Aldridge is the executive coordinator and director at Alliance for Natural Health International.
