






Off the top, I’m going to publish hard-to-find information that vaccine industry interests have forced the Centers for Disease Control and Prevention (CDC) to remove from its website.
Those interests are challenging what would be the biggest wholesale change to the childhood vaccine schedule ever. And still more changes may be to come: Robert F. Kennedy Jr.’s U.S. Department of Health and Human Services (HHS) has promised the first-ever scientific analysis of the safety profile of the entire, cumulative childhood vaccine schedule.
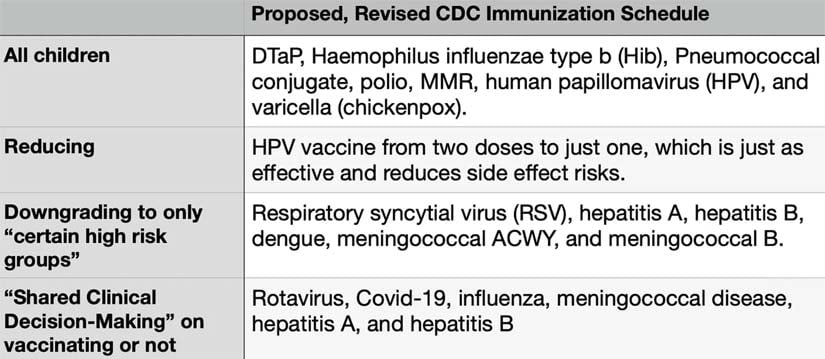
First, here are the changes the CDC tried to implement earlier this year:
Now, details, background and links to valuable information.
There isn’t a baby boom.
At least that’s what I’m told when I do a bit of research. Yet so many people I know, and their families and friends, seem to be having little ones in the past year or two and continuing on now!
With that come a lot of questions about what to do about vaccinations in an era of rapid scientific debate and evolving public health guidance. This time and place are unprecedented.
Today, new parents confront one of the most personal and anxiety-inducing decisions: whether and when to vaccinate their infants and children. Once viewed as a straightforward pillar of preventive medicine, the U.S. childhood immunization schedule has become a focal point of controversy.
Parents are finding themselves having to process conflicting information, legal challenges to federal policy changes, and calls for deeper scientific scrutiny — leaving many wondering what path best protects their child’s health without unintended risks.
Safety concerns
Questions about vaccine safety have existed — and frequently been minimized or dismissed by vaccine industry defenders — from the start.
The original version of the DPT vaccine, used widely from the 1940s, contained whole-cell pertussis (wP or DTwP) components.
This was essentially inactivated whole Bordetella pertussis bacteria. It was linked to common side effects like fever, irritability, swelling, febrile seizures (a convulsion triggered by a fever, usually above 102 F or hypotonic-hyporesponsive episodes).
When the hypotonic-hyporesponsive episodes occur, it’s typically within 48 hours of vaccination, and most commonly linked to the pertussis or whooping cough component.
In the 1970s and 1980s, controversy erupted over the whole-cell pertussis vaccine, causing rare but serious brain damage, such as encephalopathy or permanent brain injury.
Health authorities say the controversy led parents to dial back on vaccination, and that led to major pertussis outbreaks, including perhaps a dozen deaths worldwide from the disease.
To address safety concerns over the vaccine and brain damage, vaccine manufacturers developed a new, supposedly safer vaccine: containing acellular pertussis, aP or DTaP.
These use purified bacterial components (like pertussis toxin, filamentous hemagglutinin and pertactin) rather than whole cells. Whole cells are more dangerous because they include many extra irritating components that often cause stronger side effects, such as high fever and dangerous reactions.
This new and improved vaccine was introduced in the 1980s-1990s and adopted widely by the mid-1990s, with the U.S. fully switching by around 1997. Experts say this form causes significantly fewer adverse reactions and seems to work well initially.
However, evidence shows acellular vaccines don’t last as long — maybe just 2-5 years. That’s one reason why we can now see pertussis outbreaks in vaccinated people.
In other words, parents are asked to subject their children to the risk of vaccine side effects for possible short-term protection from a disease that rarely has long-lasting or serious effects — a disease that their child may never actually get.
Multiply this concern by all of the vaccines, and the entire schedule becomes a difficult sell to many parents who are doing their research.
The traditional schedule: A heavy load
Under longstanding CDC recommendations prior to recent shifts, the childhood vaccine schedule was extensive, to say the least.
Official sources and analyses indicate that following the full schedule from birth through age 18 involves giving a kid around 72 vaccine doses, including annual flu shots and accounting for COVID-19 recommendations in recent years.
This figure counts individual antigens or components separately. For example, one shot of MMR, for measles, mumps, rubella, is actually three distinct components per dose. If recommended at multiple ages (typically two doses), that multiplies accordingly.
DTaP against diphtheria, tetanus and pertussis (whooping cough) consists of three components — across a five-dose series in early childhood. That means 15 vaccine doses in five shots.
The autism connection
As we all know, autism rates have skyrocketed beyond belief, coinciding with the expansion of the vaccine schedule. While major health authorities and vaccine interests continue to claim there’s no causal link, the government has admitted and paid compensation for many cases of vaccine-induced autism, initially trying to seal and keep confidential the payments.
Testimony from whistleblowers, including a CDC senior scientist, and the government/vaccine industry’s one-time top expert witness, has further eroded trust.
They have pointed to firm links between vaccines and autism, as well as widespread efforts to cover them up.
No studies have definitively been able to rule out a link between vaccines and autism, and hundreds of scientific studies support or confirm relationships between vaccines and autism, as well as an entire range of neurological disorders such as tics and stuttering, autoimmune disorders like juvenile diabetes and Crohn’s, rashes, allergies, asthma and more.
Scientists agree that the potential culprits are manifold. Some children have a bad reaction to components in vaccines, like aluminum. Some kids have an inappropriate immune response to a vaccine rather than the desired protective response, impacting their immune system and opening the door to a host of disorders, depending on their individual predispositions.
Some babies can’t handle the assault of multiple vaccinations given at once, especially combined with other toxic exposures in their lives. Some have a bad reaction to live virus vaccines. That’s because the virus is alive and still able to replicate.
It can cause the actual disease (or a severe version of it), especially in people with weak immune systems. And babies may have unknown and undiagnosed predispositions that make them vulnerable to documented vaccine safety risks.
There is some general agreement that “vulnerable subgroups,” babies and children with genetic predispositions, family history of autoimmune issues, or mitochondrial conditions face higher risks from even a single vaccine, while many children seem to tolerate the full battery of vaccines without serious issues.
Unfortunately, our medical establishment has not taken steps to form reliable pre-vaccination screening methods to identify at-risk infants. This is despite the fact that health experts have long documented that children born with tuberous sclerosis and mitochondrial disorders are among those who seem to be at higher risk of being damaged by vaccination.
Other predispositions could be identified and screened for — but no public authority is attempting to develop such screenings. If screenings were developed, the vulnerable children could be spared, or safer vaccines developed for them.
But what to do?
Enter Kennedy, appointed as U.S. health secretary. Long a vocal critic of certain vaccine policies, Kennedy is possibly the most well-informed political figure on the issue, having not only studied it but successfully litigated vaccine injury cases as an attorney.
Kennedy has advocated for a rigorous, independent scientific review of the entire childhood vaccine schedule. It would be the first of its kind. While Google searches return the refrain that vaccines are the most widely tested and proven products on the planet, that simply isn’t true.
The cumulative effects, timing, aluminum content and comparisons to schedules in countries like Denmark, Japan or Germany, which often recommend fewer routine vaccines, have never been done. Strike that — if it’s been done, the results haven’t been publicly released.
Under Kennedy’s leadership, the CDC took groundbreaking action. It moved toward a revised schedule reducing universal recommendations from around 17-18 diseases to 11 core ones. Vaccine recommendations for flu, rotavirus (causing diarrhea), hepatitis A and B, and others shifted to “shared clinical decision-making” or for high-risk kids only.
This overhaul aimed to align with international practices and reduce adverse events, while preserving access for parents who choose to continue to opt for the full 72.
However, these proposed changes faced immediate pushback from establishment medical groups, including the American Academy of Pediatrics, which is heavily funded and influenced by the pharmaceutical industry.
Lawsuits filed against the government allege there were procedural violations in restructuring the Advisory Committee on Immunization Practices and making the new recommendations.
Federal judges have issued blocks, temporarily restoring prior guidance and pausing implementation of the new, scaled-down vaccine schedule.
Here are the changes Kennedy’s HHS proposed:
Continued recommendation for all children to get DTaP, Haemophilus influenzae type b (Hib), Pneumococcal conjugate, polio, MMR, human papillomavirus (HPV) and varicella (chickenpox).
Reducing the HPV vaccine from two doses to one, which is just as effective and reduces side effect risk.
Downgraded to only “certain high risk groups” should get: respiratory syncytial virus (RSV), hepatitis A, hepatitis B, dengue, meningococcal ACWY and meningococcal B.
To be considered to give or skip under “Shared Clinical Decision-Making”: rotavirus, COVID-19, influenza, meningococcal disease, hepatitis A and hepatitis B.
Money at stake
Billions of industry and taxpayer dollars are at stake.
When a vaccine falls off the universally recommended schedule, it means that government insurance for the poor, Medicaid, and possibly other insurers, will no longer cover the cost.
This means a “golden goose” for a vaccine maker— a blockbuster drug — could become almost instantly near-worthless based on these changes.
Expect pharmaceutical companies, and many in the media whom they largely control by funding advertising, to take positions against altering the vaccine schedule or to conduct scientific reviews of its safety.


No one-size-fits-all
Health experts across perspectives agree: individual biology varies. Some vaccines are more necessary than others. Some are safer than others. Some children have a biology that allows them to handle the full schedule without issue; others may become sick with short-term or chronic disorders, become brain damaged or even die.
Without reliable predictive tools for vaccine injury risk, parents and doctors are left to try to weigh family history, local disease prevalence and personal values.
However, as I documented in my national bestseller “Follow the Science,” doctors are frequently taught misleading or incorrect information in medical school and continuing medical education classes, due to vaccine industry influence over the material.
Right now, pediatricians often recommend following the longstanding, court-restored CDC guidance. But some skeptics urge spacing out shots, delaying certain shots or getting exemptions entirely.
In this climate of legal challenges and policy flux, the best approach likely involves thorough research, open discussions with your trusted doctors and truly informed consent, which is often lacking.
‘Turtles All the Way Down’
One influential text in these debates is “Turtles All the Way Down: Vaccine Science and Myth” (edited by Zoey O’Toole and Mary Holland, published anonymously by a team of researchers).
I conducted an interview about the book for my podcast, “The Sharyl Attkisson Podcast.” The title draws from an ancient cosmological metaphor implying a chain of reasoning or causes that goes backward forever, meaning you can never find a starting point or a final explanation.
The book states that vaccine safety testing has lacked a critical comparison component: true inert placebos like saline. Can you imagine? The safety impact of a vaccine isn’t tested against not getting the vaccine.
Instead, new vaccines are frequently compared to earlier vaccines or formulations containing similar adjuvants and components minus the target antigen. This creates a chain where safety is never benchmarked against a neutral control — hence “turtles all the way down.”
The book exposes flawed trial designs, post-licensure surveillance limitations and the absence of large-scale studies on the full schedule’s combined effects. The authors call for better placebo-controlled trials and individualized risk assessment.
Proposed changes (currently under court challenge)
Here are the changes that Kennedy’s HHS proposed (under challenge from vaccine industry advocates):
- Continued recommendation for all children to get DTaP, Hib, Pneumococcal conjugate, polio, MMR, HPV and varicella (chickenpox).
- Reducing the HPV vaccine from two doses to one, which is just as effective and reduces side effect risk.
- Downgraded to “only for certain high risk groups”: respiratory syncytial virus (RSV), hepatitis A, hepatitis B, dengue, meningococcal ACWY and meningococcal B.
- To be considered to give or skip under “Shared Clinical Decision-Making”: rotavirus, COVID-19, influenza, meningococcal disease, hepatitis A and hepatitis B.
Here is the proposed schedule in chart form, since removed from the HHS website, showing the ages and doses recommended.
Bottom line
My own child was fully vaccinated: I hadn’t yet been assigned to cover vaccine controversies at CBS News when she was little. With today’s knowledge, would I do things differently? Yes. But, obviously, I cannot give medical advice on a topic that is very driven by individuality.
Until the government comes through with its next stage of evidence-based recommendations, here is some information from others. It’s important that you make your own decisions that are best for your own family.
From a highly placed medical doctor and official.
“I think that parents should read the ‘Turtles All the Way Down book.’ It is the best resource I’ve seen that provides a an unbiased and informative perspective. The problem as you know is that a lot of the science is totally corrupted so it puts parents and families in a terrible position.
“And the corruption leads to obfuscation of risk and usually just neglect of robust risk analysis. So while a vaccine might be effective for the condition it targets, there are all of these other effects for which there’s been almost no interest in examining properly.
“I personally have zero confidence in the main resources like the historical CDC that have guided this area. But on the other side of that not every family is really comfortable actually sticking with their decision, which suggests that they may not have made the right one for themselves in the first place.
“For example, if a family opts out of the measles vaccine, but then a year later races to get measles shots when they hear about an outbreak, they probably didn’t make an informed decision the first time around. That’s why I think the book is so good, helps people make an informed decision the first time around.”
From another medical advocate:
“We don’t give a guide on any alternative schedule. The reason is that there is no way to determine in advance what child might have a reaction to a vaccine. And any vaccine could potentially be harmful.
“We do recommend that if a parent is thinking of doing some, they need to do only one at a time and avoid combination vaccines. And space them out by at least 2 or 3 months. And to make sure their child is healthy and watch them carefully for potential side effects.”
Other specific notes from medical experts:
“Hep B is unnecessary at birth and has a higher adverse event profile than other childhood vaccines.”
“Gardasil is problematic, and according to the inventor herself, risks may outweigh any benefits.”
“It’s better to get chicken pox than to get a vaccine that has limited effectiveness and may simply postpone chicken pox until a child is older and cases are considered more serious. The vaccine is linked in some studies to shingles, though vaccine advocates dispute this.”
“Covid vaccine is unnecessary for healthy people, doesn’t work well, has side effects, and could be especially problematic in people with predisposition for health issues.”
“If you must give DTaP, consider option out of the ‘P’ part (pertussis, whooping cough), which is particularly problematic.”
“Flu vaccines are unnecessary for children, ineffective in adults, associated with a higher death rate in senior, and contain potentially harmful adjuvants.”
- The National Vaccine Information Center is a terrific resource.
- HHS memo recommending changes to vaccine schedule.
- HHS fact sheet on changing vaccine schedule.
Official vaccine side effect information
FDA package inserts
Immunize.org FDA Package Inserts — Alphabetical list with direct PDFs for every vaccine (DTaP, MMR, polio, Hep B, etc.). Filter by vaccine name. You can download the full insert for each childhood vaccine and extract the “Adverse Reactions” or “Postmarketing Experience” sections.
CDC summary of possible side effects
CDC, Possible Side Effects from Vaccines — This pulls directly from Vaccine Information Statements (VIS) and package inserts. It covers common and rare events by vaccine type.
Vaccine Injury Compensation Program table
Vaccine Injury Table — This lists injuries/conditions presumed compensable (with time frames) for covered childhood vaccines. It is not a full adverse event list, but a legal reference for serious events.
Individual manufacturer inserts — Search any vaccine on FDA Vaccines Licensed for Use in the United States.
VAERS, Vaccine Adverse Event Reporting System
vaers.hhs.gov — Public database for observed events after vaccination. All illnesses after vaccination should be reported so that experts can detect formerly unknown patterns. Not all illnesses are connected to vaccination, but only by collecting all reports can the database reveal previously unknown side effects. Experts say vaccine adverse events can happen months or years after vaccination.
Additional resources
- Current CDC vaccine schedule.
- Sharyl Attkisson stories and resources here (including on Gardasil, flu shots, autism).
- Dr. Andrew Zimmerman’s affidavit on vaccine-autism link and government cover-up. Zimmerman was the government and vaccine industry’s expert witness when he came to discover “vaccines can — and do — cause autism, after all.”
- CDC senior scientist alleges vaccine-autism link and cover-up that he took part in with colleagues.
- Example of research linking vaccines to food allergies.
- Document in Poling case where government admitted vaccination caused the child’s autism, but then the government had the records sealed so other parents wouldn’t know, and continued to publicly state the link was a “myth” or “conspiracy theory.”
- My news report on the Poling case when it leaked out to the public.
- Nine more cases of the government paying settlements for vaccine-autism injuries.
- Former head of NIH, Dr. Bernadine Healy, stated that her colleagues were intentionally diverting from the vaccine-autism question.
- Conflicts of interest among vaccine defenders such as the American Academy of Pediatrics, Every Child By Two* (now “Vaccinate Your Family”) and Dr. Paul Offit.
- *While Rosalynn Carter and Betty Bumpers served as the public faces and supposed co-founders of Every Child By Two, as I revealed in my reporting, the administrative and financial infrastructure was heavily driven by the industry from day one.
- The Glaxo executive liaison: For years, William Engesser, a top executive and director of government relations for GlaxoSmithKline (GSK), served as the treasurer on the board of directors for Every Child By Two. Having a high-ranking pharmaceutical executive manage the financial books and serve as treasurer of an ostensibly independent public health nonprofit classifies it as an industry front group.
- Millions in seed funding: Form 990 filings and corporate transparency disclosures confirm that GSK, along with Merck, Sanofi Pasteur, and Wyeth — all top vaccine makers — provided the literal financial foundation (amounting to millions over the years) that kept the organization running.
Originally published on Sharyl Attkisson’s Substack page.
