


Miss a day, miss a lot. Subscribe to The Defender's Top News of the Day. It's free.
In an article published Feb. 7, The Exposé reported Pfizer’s COVID-19 vaccine “increases children’s risk of death 5100%,” based on data recorded by the UK’s Office for National Statistics (ONS).
The ONS is the UK’s largest independent producer of official statistics that include COVID vaccine uptake and mortality by age group.
The ONS data cited by The Exposé is found in table 9 of the dataset, labeled “Deaths occurring between 1 January 2021 and 31 October 2021 edition of this dataset.” It can be downloaded directly from the ONS website here.
The Exposé accurately plotted some of the ONS data in its article:

As the above table shows, the all-cause mortality rate in the doubly vaccinated is in fact 238.7/4.58 = 52 times larger, or 5,100% higher than in the unvaccinated.
However, before drawing any conclusions it is imperative to examine the actual ONS data more closely.
First, we must consider the total number of deaths in each population. There were 96 total deaths among nearly 2.1 million unvaccinated children in the 10- to 14-year-old age group compared to four deaths among 1,678 children in that age group who had received their second dose 21 days or more prior to their demise.
Children who received only one dose or who were inside the 21-day window were not included in the subgroup with the highest mortality.


The Exposé chose to compare the most extreme subset of the vaccinated to support its provocative headline. Moreover, although the specific cause of death is not given (the ONS only separates cause of death into COVID or non-COVID-related), none of the four deaths were related to COVID.
This poses important questions. What if the four perished in an automobile accident? What if they were all suffering from a debilitating chronic condition that led to a predictable fatality?
We arrive at a major confounder: These two populations of children are not necessarily matched.
It is likely parents with children with significant comorbidities would have more readily sought the vaccine for their kids compared to parents with healthy children.
According to actuarial tables from the U.S. Social Security Administration, the risk of death in a 10- to 14-year-old is about 1 to 1.7 in 10,000 in a given year.
These numbers are 2 to 4 times higher than the mortality rate in the unvaccinated group in the ONS dataset, further indicating that this group is healthier than the average.
Nevertheless, taking all children who had received at least one dose of the vaccine as a whole, we find that 11 deaths occurred in 27,359 person-years. This mortality rate is still significantly higher (nearly 9 times) than the unvaccinated.
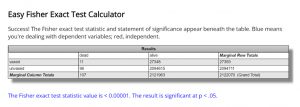
Based on the Fisher Exact Test — a standard statistical test used to determine if the proportions of categories in two group variables significantly differ from each other — there is less than a 1 in 100,000 probability this difference could have happened at random.
What do ONS data reveal about vaccine effectiveness?
As stated above, though a large difference in mortality between the vaccinated and unvaccinated exists, it is impossible, based on ONS data, to come to any definitive conclusions about the safety of these vaccines because of the mismatched cohorts and the small number of unclassified deaths in one of the groups.
Let us now examine what this data may tell us about the effectiveness of the shots. How good are the vaccines at preventing deaths from COVID in this age group?
There were two COVID deaths in 2,121,963 unvaccinated person-years. There were also two COVID deaths in 27,359 vaccinated person-years.
This means the vaccine effectiveness (VE) = -7,557%. This is because the unvaccinated group is 76.57 times larger and had the same number of deaths due to COVID.
However, the deaths in the vaccinated group occurred before the child had received a second dose.
By Pfizer’s methodology, blessed by the U.S. Food and Drug Administration (FDA), its product is 100% effective. This is a direct result of only counting deaths 14 days after the second dose.
With “zero” deaths in the vaccinated and two in the unvaccinated, the vaccine is 100% effective in preventing death from COVID.
On the other hand, if we compare the two groups of adolescents aged 15-19, we find that there was one COVID death in the 127,842 person-years of the fully vaccinated group and 18 in the 1,587,072 person-years of the unvaccinated group. This results in a calculated vaccine effectiveness of only 31%.
Where does that leave us?
The ONS data give us much to be concerned about. There seems to be an undeniable safety signal emerging from England which must be monitored closely over time.
Strangely enough, the subsequent data set from the ONS, which includes data through the end of December 2021, conspicuously excludes children in these age groups.
Where else, then, can we look? The Centers for Disease Control and Prevention has chosen not to report on deaths by vaccination status in this age group.
We are in the same predicament that Pfizer’s severely flawed and underpowered pediatric trial left us in. With fewer than 2,200 children involved and only 1,450 receiving the vaccine, the trial did not answer any questions about safety or efficacy.
Dr. Eric Rubin, editor-in-chief of the New England Journal of Medicine and member of the FDA’s vaccine advisory panel, acknowledged the trial did not offer any information by succinctly and notoriously stating during an FDA hearing, “We are never going to learn how safe this vaccine is until we start giving it. That’s just the way it is.”
Rubin is not completely correct. We could learn how safe this vaccine is if he and his fellow advisory panel members demanded that a properly powered and designed trial were conducted prior to deploying the vaccine to tens of millions of children.
In any case, we have started giving it. When will we learn how safe this vaccine is?
More importantly, what should we do in the meantime? Pause childhood vaccinations until data can be collected and deaths investigated?
Or carry on while testing it on infants 6 months of age and older?
